
Physical Development
After this chapter, you should be able to:
- Explain the changes in physical growth and brain growth
- Compare and contrast different male and female changes that occur during puberty
- Discuss teenage pregnancy, birth control, and sexual health
- Summarize adolescent health: sleep, diet, and exercise
- Explain the prevalence, risk factors, and consequences of adolescent pregnancy and sexual health
- Describe factors contributing to increased mental health issues for adolescence
- Identify symptoms and treatment approaches associated with select mental health disorders
PHYSICAL GROWTH
The adolescent growth spurt is a rapid increase in an individual’s height and weight during puberty resulting from the simultaneous release of growth hormones, thyroid hormones, and androgens. Males experience their growth spurt about two years later than females. The accelerated growth in various body parts happens at different times, but for all adolescents it has a fairly regular sequence. The first places to grow are the extremities (head, hands, and feet), followed by the arms and legs, and later the torso and shoulders. This non-uniform growth is one reason why an adolescent body may seem out of proportion. During puberty, bones become harder and more brittle.
Before puberty, there are nearly no differences between biological males and females in the distribution of fat and muscle. During puberty, males grow muscle much faster than females, and females experience a higher increase in body fat. An adolescent’s heart and lungs increase in both size and capacity during puberty; these changes contribute to increased strength and tolerance for exercise.[1]
 |
 |
Video reviews what growth spurts are and offers advice for adolescents to promote healthy growth
BRAIN GROWTH
Brain Growth continues into the early 20s. The development of the frontal lobe, in particular, is important during this stage. Adolescents often engage in increased risk-taking behaviors and experience heightened emotions during puberty; this may be due to the fact that the frontal lobes of their brains—which are responsible for judgment, impulse control, and planning—are still maturing until early adulthood (Casey, Tottenham, Liston, & Durston, 2005)
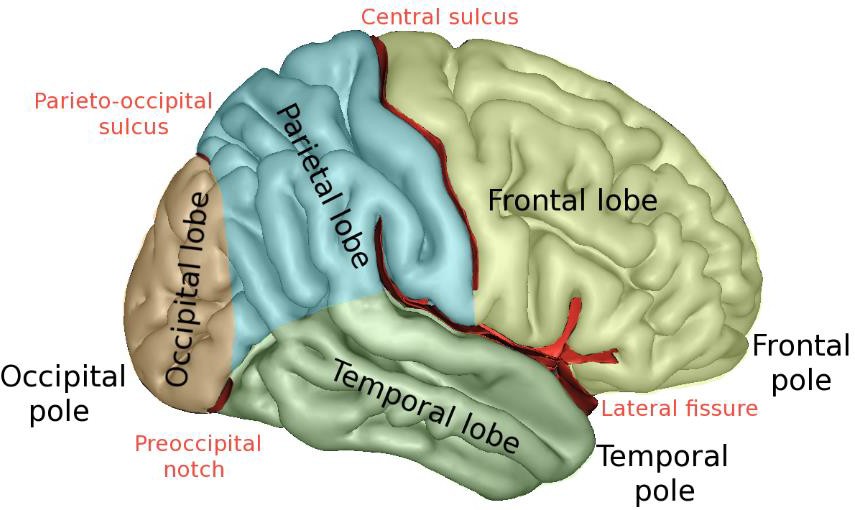
The brain undergoes dramatic changes during adolescence. Although it does not get larger, it matures by becoming more interconnected and specialized (Giedd, 2015). The myelination and development of connections between neurons continues. This results in an increase in the white matter of the brain, and allows the adolescent to make significant improvements in their thinking and processing skills. Different brain areas become myelinated at different times. For example, the brain’s language areas undergo myelination during the first 13 years. Completed insulation of the axons consolidates these language skills but makes it more difficult to learn a second language. With greater myelination, however, comes diminished plasticity as a myelin coating inhibits the growth of new connections (Dobbs, 2012).
Even as the connections between neurons are strengthened, synaptic pruning occurs more than during childhood as the brain adapts to changes in the environment. This synaptic pruning causes the gray matter of the brain, or the cortex, to become thinner but more efficient (Dobbs, 2012). The corpus callosum, which connects the two hemispheres, continues to thicken, allowing for stronger connections between brain areas. Additionally, the hippocampus becomes more strongly connected to the frontal lobes, allowing for greater integration of memory and experiences into our decision-making.[1]
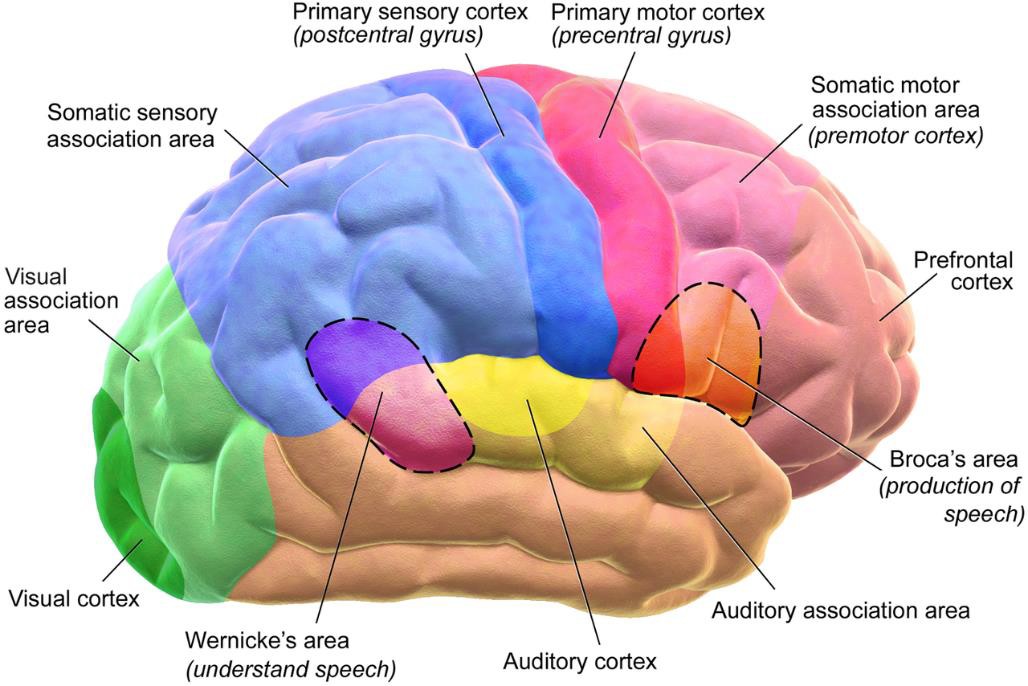
The limbic system, which regulates emotion and reward, is linked to the hormonal changes that occur at puberty. The limbic system is also related to novelty seeking and a shift toward interacting with peers. In contrast, the prefrontal cortex, which is involved in the control of impulses, organization, planning, and making good decisions, does not fully develop until the mid-20s. According to Giedd (2015) the significant aspect of the later developing prefrontal cortex and early development of the limbic system is the “mismatch” in timing between the two. The approximately ten years that separates the development of these two brain areas can result in risky behavior, poor decision-making, and weak emotional control for the adolescent. When puberty begins earlier, this mismatch extends even further.
Teens often take more risks than adults and, according to research, it is because they weigh risks and rewards differently than adults do (Dobbs, 2012). For adolescents, the brain’s sensitivity to the neurotransmitter dopamine peaks, and dopamine is involved in reward circuits so the possible rewards outweigh the risks. Adolescents respond especially strongly to social rewards during activities, and they prefer the company of others their same age. In addition to dopamine, the adolescent brain is affected by oxytocin, which facilitates bonding and makes social connections more rewarding. With both dopamine and oxytocin engaged, it is no wonder that adolescents seek peers and excitement in their lives that could end up actually harming them.
Because of all the changes that occur in the adolescent brain, the chances for abnormal development can occur, including mental illness. In fact, 50% of mental illness occurs by the age 14 and 75% occurs by age 24 (Giedd, 2015). Additionally, during this period of development the adolescent brain is especially vulnerable to damage from drug exposure. For example, repeated exposure to marijuana can affect cellular activity in the endocannabinoid system. Consequently, adolescents are more sensitive to the effects of repeated marijuana exposure (Weir, 2015).
However, researchers have also focused on the highly adaptive qualities of the adolescent brain, which allow the adolescent to move away from the family towards the outside world (Dobbs, 2012; Giedd, 2015). Novelty seeking and risk taking can generate positive outcomes including meeting new people and seeking out new situations. Separating from the family and moving into new relationships and different experiences are actually quite adaptive for society.[2]

Video briefly reviews how changes in the brain during adolescence can contribute to risk-taking behavior.
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- An Introduction to Nutrition- Nutrition through the Life Cycle: From Pregnancy to the Toddler Years by Maureen Zimmerman and Beth Snow is licensed under CC BY-NC-SA 3.0 ↵
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 (modified by Courtney Boise) ↵
PHYSICAL CHANGES IN ADOLESCENCE
The physical growth and the changes of puberty mark the onset of adolescence (Lerner & Steinberg, 2009). For both boys and girls, these changes include a growth spurt in height, growth of pubic and underarm hair, and skin changes (e.g., pimples). Hormones drive these pubescent changes, particularly the increase in testosterone for biological males and estrogen for biological females.[1] Puberty is a developmental period in which hormonal changes cause rapid physical alterations in the body, culminating in sexual maturity. Although the timing varies to some degree across cultures, the average age range for reaching puberty is between 9 and 14 years for biological females and between 10 and 17 years for biological males (Marshall & Tanner, 1986). This period of physical development of the adolescent age 9-13 is divided into two phases.[2]
The first phase of puberty begins when the pituitary gland begins to stimulate the production of the male sex hormone testosterone in biological males and the female sex hormones estrogen and progesterone in biological females. The release of these sex hormones triggers the development of the primary sex characteristics, the sex organs concerned with reproduction. It also involves height increases from 20 to 25 percent. Puberty is second to the prenatal period in terms of rapid growth as the long bones stretch to their final, adult size. Biological females grow 2–8 inches (5–20 centimeters) taller, while biological males grow 4–12 inches (10–30 centimeters) taller.
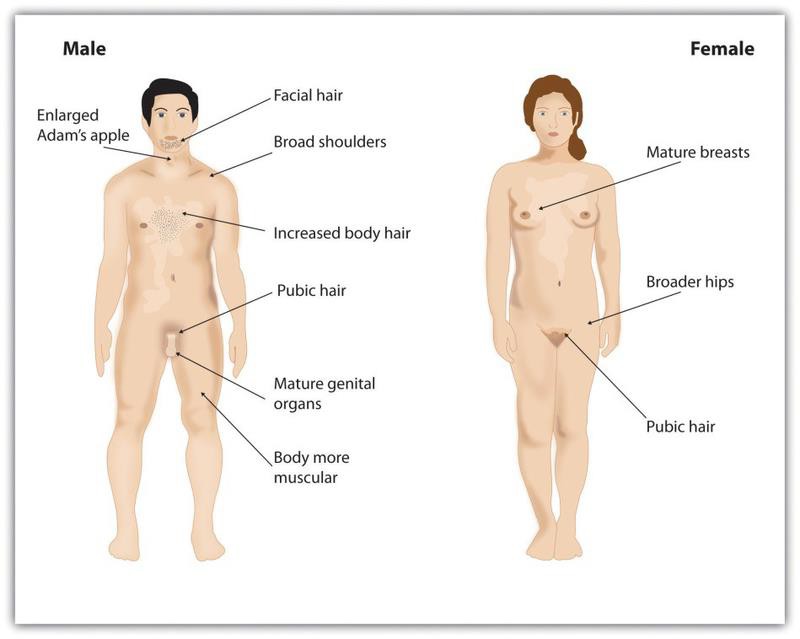
Secondary sexual characteristics are visible physical changes not directly linked to reproduction but signal sexual maturity. The growth spurt for biological females usually occurs earlier than that for biological males, with some males continuing to grow into their 20s. For males this includes broader shoulders, an enlarged Adam’s apple, and a lower voice as the larynx grows. Biological males typically begin to grow facial hair between ages 14 and 16, which becomes coarser and darker, and hair growth occurs in the pubic area, under the arms, and on the face.
For biological females the enlargement of breasts is usually the first sign of puberty and, on average, occurs between ages 10 and 12 (Marshall & Tanner, 1986). Their hips broaden and pubic and underarm hair develops and becomes darker and coarser. Adolescents regardless of gender experience a rapid growth spurt during this stage. Adolescents may begin shaving during this time period as well as showing signs of acne on their faces and bodies.

Acne is an unpleasant consequence of the hormonal changes in puberty. Acne is defined as pimples on the skin due to overactive sebaceous (oil-producing) glands (Dolgin, 2011). These glands develop at a greater speed than the skin ducts that discharge the oil. Consequently, the ducts can become blocked with dead skin and acne will develop. According to the University of California at Los Angeles Medical Center (2000), approximately 85% of adolescents develop acne, and biological males develop acne more than biological females because of greater levels of testosterone in their systems (Dolgin, 2011). Hormones that are also responsible for sexual development can also wreak havoc on the teenage skin.[3]
A major milestone in puberty for biological females is menarche, the first menstrual period, typically experienced at around 12 or 13 years of age (Anderson, Dannal, & Must, 2003). The age of menarche varies substantially and is determined by genetics, as well as by diet and lifestyle, since a certain amount of body fat is needed to attain menarche. Biological females who are very slim, who engage in strenuous athletic activities, or who are malnourished may begin to menstruate later. Even after menstruation begins, individuals whose level of body fat drops below the critical level may stop having their periods. The sequence of events for puberty is more predictable than the age at which they occur. Some biological females may begin to grow pubic hair at age 10 but not attain menarche until age 15.[4]
Male Anatomy
Biological males have both internal and external genitalia that are responsible for procreation and sexual intercourse. Biological males produce their sperm on a cycle, and unlike the biological female’s ovulation cycle, the male sperm production cycle is constantly producing millions of sperm daily. The male sex organs are the penis and the testicles, the latter of which produce semen and sperm. The semen and sperm, as a result of sexual intercourse, can fertilize an ovum in the female’s body; the fertilized ovum (zygote) develops into a fetus, which is later born as a child.

https://youtube.com/watch?v=G2ciOhidKpg%3Ffeature%3Doembed%26rel%3D0
Video reviews male reproductive organs.
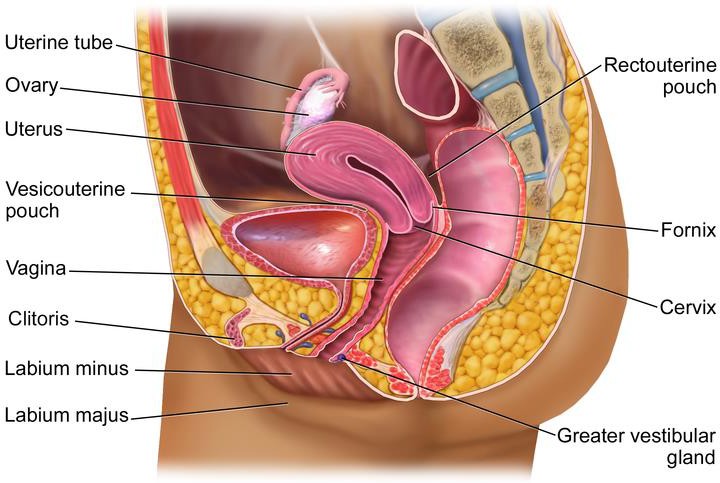
Female Anatomy
External genitalia for biological females is collectively known as the vulva, which includes the mons veneris, labia majora, labia minora, clitoris, vaginal opening, and urethral opening. Female internal reproductive organs consist of the vagina, uterus, fallopian tubes, and ovaries. The uterus hosts the developing fetus, produces vaginal and uterine secretions, and passes the male’s sperm through to the fallopian tubes while the ovaries release the eggs. A biological female is born with all eggs already produced. The vagina is attached to the uterus through the cervix, while the uterus is attached to the ovaries via the fallopian tubes. Biological females have a monthly reproductive cycle; at certain intervals the ovaries release an egg, which passes through the fallopian tube into the uterus. If, in this transit, it meets with sperm, the sperm might penetrate and merge with the egg, fertilizing it. If not fertilized, the egg and the tissue that was lining the uterus is flushed out of the system through menstruation (around every 28 days).
Video reviews female reproductive organs.
Effects of Puberty on Development
The age of puberty is getting younger for children throughout the world. A century ago the average age of an individual’s first period in the United States and Europe was 16, while today it is around 13. Because there is no clear marker of puberty for biological males, it is harder to determine if they are maturing earlier, too. In addition to better nutrition, less positive reasons associated with early puberty for biological females include increased stress, obesity, and endocrine disrupting.
Because rates of physical development vary so widely among teenagers, puberty can be a source of pride or embarrassment. Individuals who develop more slowly than their peers may feel self-conscious about their lack of physical development; some research has found that negative feelings are particularly a problem for late maturing biological males, who are at a higher risk for depression and conflict with parents (Graber et al., 1997) and more likely to be bullied (Pollack & Shuster, 2000). Additionally, problems are more likely to occur when the child is among the first in his or her peer group to develop. Because the preadolescent time is one of not wanting to appear different, early developing children stand out among their peer group and gravitate toward those who are older (Weir, 2016).
Early maturing biological males tend to be physically stronger, taller, and more athletic than their later maturing peers; this can contribute to differences in popularity among peers, which can in turn influence the teenager’s confidence. Some studies show that males who mature earlier tend to be more popular and independent but are also at a greater risk for substance abuse and early sexual activity (Flannery, Rowe, & Gulley, 1993; Kaltiala-Heino, Rimpela, Rissanen, & Rantanen, 2001).
Early maturing biological females may face increased teasing and sexual harassment related to their developing bodies, which can contribute to self-consciousness and place them at a higher risk for anxiety, depression, substance abuse, and eating disorders (Ge, Conger, & Elder, 2001; Graber, Lewinsohn, Seeley, & Brooks-Gunn, 1997; Striegel-Moore & Cachelin, 1999).[5]
Video reviews pubertal changes across multiple areas of physical development for individuals who’s biological sex is female.
- Adolescent Development by Jennifer Lansford is licensed under CC BY-NC-SA 4.0 ↵
- Adolescence: Developing Independence and Identity by Charles Stangor is licensed under CC BY-NC-SA 3.0; ↵
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0; ↵
- Adolescence: Developing Independence and Identity by Charles Stangor is licensed under CC BY-NC-SA 3.0; ↵
- Adolescence Physical Growth by Boundless.com is licensed under CC BY-SA 4.0; Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 (all sections modified by Courtney Boise) ↵
ADOLESCENT HEALTH: SLEEP, DIET, AND EXERCISE
Sleep Health
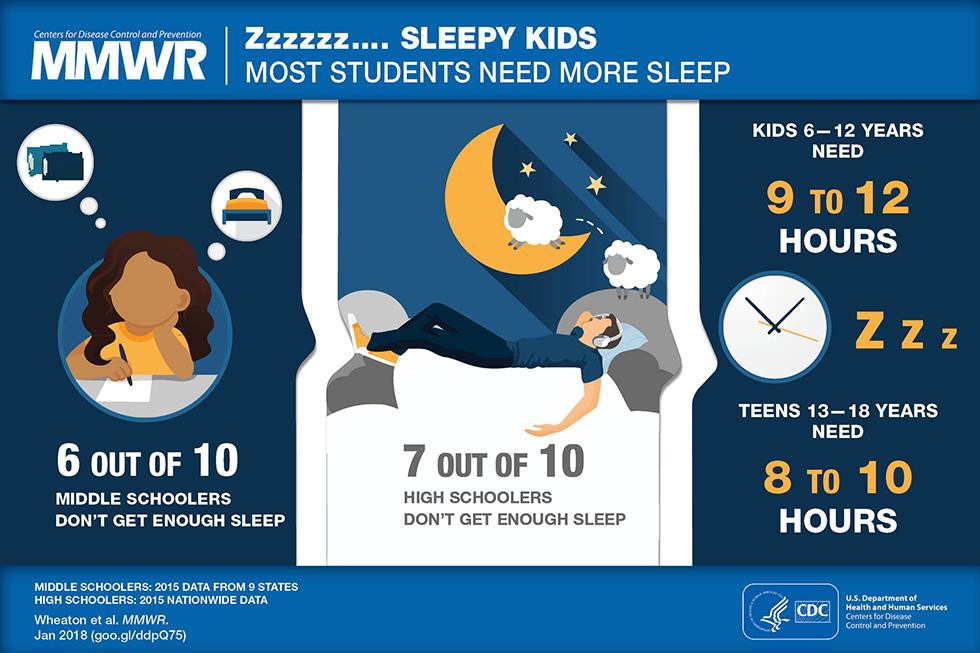
According to the National Sleep Foundation (NSF) (2016), adolescents need about 8 to 10 hours of sleep each night to function best. The most recent Sleep in America poll in 2006 indicated that adolescents between sixth and twelfth grade were not getting the recommended amount of sleep. For the older adolescents, only about one in ten (9%) get an optimal amount of sleep, and they are more likely to experience negative consequences the following day. These include feeling too tired or sleepy, being cranky or irritable, falling asleep in school, having a depressed mood, and drinking caffeinated beverages (NSF, 2016). Additionally, they are at risk for substance abuse, car crashes, poor academic performance, obesity, and a weakened immune system (Weintraub, 2016).
Why don’t adolescents get adequate sleep? In addition to known environmental and social factors, including work, homework, media, technology, and socializing, the adolescent brain is also a factor. As adolescents go through puberty, their circadian rhythms change and push back their sleep time until later in the evening (Weintraub, 2016). This biological change not only keeps adolescents awake at night, it makes it difficult for them to get up in the morning. When they are awake too early, their brains do not function optimally. Impairments are noted in attention, behavior, and academic achievement, while increases in tardiness and absenteeism are also demonstrated. Psychologists and other professionals have been advocating for later school times, and they have produced research demonstrating better student outcomes for later start times. More middle and high schools have changed their start times to better reflect the sleep research.[1]

Video reviews how adolescents circadian rhythms change, the importance of sleep, and tips for getting adequate sleep.
Eating: Healthy Habits = Healthy Lives
The Dietary Guidelines define late adolescence, as the period from ages fourteen to eighteen. After puberty, the rate of physical growth slows down. Biological females stop growing taller around age sixteen, while biological males continue to grow taller until ages eighteen to twenty. One of the psychological and emotional changes that take place during this life stage includes the desire for independence as adolescents develop individual identities apart from their families. As teenagers make more of their dietary decisions, parents, caregivers, and authority figures should guide them toward appropriate, nutritious choices.

Some adolescents don’t have all the food necessary for proper development and may be food insecure. Most people have access to fresh water in all except the most extreme situations; the need for food is the most fundamental and important human need. More than 1 in 10 U.S. households contain people who live without enough nourishing food and this lack of proper nourishment has profound effects on their abilities to lead lives that will allow them to develop to their fullest potential. (Hunger Notes, n.d.).
When people are extremely hungry, their motivation to attain food completely changes their behavior. Hungry people become listless and apathetic to save energy and then become completely obsessed with food. Ancel Keys and his colleagues (Keys, Brožek, Henschel, Mickelsen, & Taylor, 1950) found that volunteers who were placed on severely reduced-calorie diets lost all interest in sex and social activities, becoming preoccupied with food.[2]
Healthy Habits
Forming good eating habits and engaging in fitness or exercise programs will help promote lifelong healthy habits.
The energy (calorie) requirements for preteens differ according to gender, growth, and activity level. For ages nine to thirteen, females should consume about 1,400 to 2,200 calories per day and males should consume 1,600 to 2,600 calories per day. Physically active preteens who regularly participate in sports or exercise need to eat a greater number of calories to account for increased energy expenditures.
Exercise improves our overall mental health by lowering stress and improving feelings of well-being. Exercise also increases cardiovascular capacity, lowers blood pressure, and helps improve diabetes, joint flexibility, and muscle strength (American Heart Association, 1998). For long lasting change, it’s important to plan healthy meals, limit snacking, and to schedule exercise into our daily lives.[3]
Eating Disorders
Although eating disorders can occur in children and adults, they frequently appear during the teen years or young adulthood (National Institute of Mental Health (NIMH), 2016). Eating disorders affect multiple genders, although rates among women are 2 1⁄2 times greater than among men. An individual with an eating disorder has a distorted sense of body image, which may include body dysmorphia or an extreme concern with becoming more muscular (Hudson, Hiripi, Pope, & Kessler, 2007; Wade, Keski-Rahkonen, & Hudson, 2011).

Video reviews symptoms and causes of a rising prevalence of eating disorders for boys.
Risk Factors for Eating Disorders
Researchers are finding that eating disorders are caused by a complex interaction of genetic, biological, behavioral, psychological, and social factors (NIMH, 2016). Eating disorders appear to run in families, and researchers are working to identify DNA variations that are linked to the increased risk of developing eating disorders. Researchers have also found differences in patterns of brain activity in women with eating disorders in comparison with healthy women.
The main criteria for the most common eating disorders: Anorexia nervosa, bulimia nervosa, and binge-eating disorder are described in the Diagnostic and Statistical Manual of Mental Disorders-Fifth Edition (DSM-5)(American Psychiatric Association, 2013) and listed in Table 6.1.[4]
|
Eating Disorder |
Description |
|
Anorexia Nervosa |
|
|
Bulimia Nervosa |
|
|
Binge-Eating Disorder |
|
Health Consequences of Eating Disorders
For those suffering from anorexia, health consequences include an abnormally slow heart rate and low blood pressure, which increases the risk for heart failure. Additionally, there is a reduction in bone density (osteoporosis), muscle loss and weakness, severe dehydration, fainting, fatigue, and overall weakness. Individuals with this disorder may die from complications associated with Anorexia nervosa, which has the highest mortality rate of any psychiatric disorder.
In this video, Dr. Rachel Goldstein uses three case studies to illustrate symptoms, causes, and interventions for anorexia.
The binge and purging cycle of bulimia can affect the digestives system and lead to electrolyte and chemical imbalances that can affect the heart and other major organs. Frequent vomiting can cause inflammation and possible rupture of the esophagus, as well as tooth decay and staining from stomach acids.
In this video, Dr. Rachel Goldstein outlines a case study and then reviews the definition of bulimia nervosa, common misconceptions of the eating disorder, and approaches to treatment. Please note, Dr. Goldstein discusses how bulimia may be comorbid with suicidal ideation.
Lastly, binge eating disorder results in similar health risks to obesity, including high blood pressure, high cholesterol levels, heart disease, Type II diabetes, and gall bladder disease (National Eating Disorders Association, 2016).
In this video, Dr. Rachel Goldstein reviews features of binge eating and treatment options. Please note, Dr. Goldstein discusses how eating disorders may be comorbid with suicidal ideation.
Eating Disorders Treatment
The foundations of treatment for eating disorders include adequate nutrition and discontinuing destructive behaviors, such as purging. Treatment plans are tailored to individual needs and include medical care, nutritional counseling, medications (such as antidepressants), and individual, group, and/or family psychotherapy (NIMH, 2016).[5]
Video briefly defines eating disorders, outlines some treatment options, and discusses why it can be difficult to recognize and treat eating disorders.

In the next section we will be looking at various psychological disorders. Learning about and supporting others seeking help when they have a mental health problem is just as important as seeking help when one is experiencing negative physical health problems.[6]
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- Nutrition through the Life Cycle: From Pregnancy to the Toddler Years by Maureen Zimmerman and Beth Snow is licensed under CC BY-NC-SA 3.0(modified by Dawn Rymond) ↵
- Beginning Psychology – Two Fundamental Human Motivations: Eating and Mating by Charles Stangor is licensed under CC BY-NC-SA 3.0 ↵
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- Lifespan Development: A Psychological Perspective by Martha Lally and Suzanne Valentine-French is licensed under CC BY-NC-SA 3.0 ↵
- 4Child Growth and Development by Jennifer Paris, Antoinette Ricardo, & Dawn Rymond licensed under CC BY 4.0 (sections modified by Courtney Boise) ↵
MAINTAINING EMOTIONAL HEALTH
Emotional regulation is the ability to successfully control our emotions, which takes effort, but the ability to do so can have important positive health outcomes. Emotional responses such as the stress reaction are useful in warning us about potential danger and in mobilizing our response to it, so it is a good thing that we have them. However, we also need to learn how to control and regulate our emotions, to prevent them from letting our behavior get out of control.[1]
Stress may not be a disorder, but if it continues and becomes more intense and debilitating, it may lead to a disorder. We experience stress in our everyday lives, including daily hassles.
People who experience strong negative emotions as a result of these hassles, exhibit negative stress responses. Stress can be managed by using coping strategies and by becoming better at emotional regulation. The best antidote for stress is to think positively, have fun, and enjoy the company of others. People who express optimism, self-efficacy, and grit tend to cope better with stress and experience better health overall.[2]
- Beginning Psychology – Stress: The Unseen Killer by Charles Stangor is licensed under CC BY-NC-SA 3.0 ↵
- Beginning Psychology – Chapter Summary by Charles Stangor is licensed under CC BY-NC-SA 3.0 ↵

{kind=link}
.png){kind=link}
{kind=link}