
11 Articulations Lab
"Nothing happens until something moves. When something vibrates, the electrons of the entire universe resonate with it. Everything is connected." -Albert Einstein
Gillian Backus; Heidi W. Wangerin; and Paula Rodgers
Objectives
- Define the terms on the terminology checklist and apply these terms to specific joints, including the knee joint.
- Define and demonstrate the different types of movements possible at synovial joints.
- Name the structural components of a typical synovial joint.
- Given an image (or description) of a joint position, determine the joint movement (or description), articulating bones, (and muscle action if muscles have been covered).
Terminology Checklist
Structural Classification of Synovial Joints
|
Structure of a Synovial Joint
|
Specific Movements at Synovial Joint
|
Synovial Joints of the Body
|
Knee Joint
|
Outline of Lab
Case Study: “The Case of the Wobbly Gymnast”
Activity 1: Classification of Joints
Activity 2: Body in Motion
Putting it All Together
Case Study: “The Case of the Wobbly Gymnast”
You are a pediatrician at a sports medicine practice. Your next patient is a 12-year-old gymnast. When she dismounted the balance beam during practice, she landed and inverted her right ankle. She has bruising around the lateral aspect of her right ankle, swelling and acute pain around her lateral malleolus, and limited range of motion. She is concerned that she has fractured her ankle and asks you about some common ankle injuries (Figure 1).
You tell her that these symptoms may suggest a sprain, a strain, or a fracture. Sprains and strains involve the stretching of the ligaments, tendons and muscles supporting a joint. A fracture involves the breaking of a bone, and they tend to occur at the joint. A less common injury is a high ankle sprain, also referred to as syndesmotic injury. A syndesmosis is a fibrous joint that unites the tibia and fibula by a sheet of connective tissue called the interosseous membrane. In a high ankle sprain, the interosseous membrane is overstretched which causes pain and instability between the tibia and fibula. You explain that ankle injuries are quite common and can range from mild to severe. Moreover, inversion injuries (rolling the ankle outward) are much more common than eversion injuries (rolling the ankle inward) because the medial side of the ankle is more stable due to the large deltoid ligament and the presence of the bony medial malleolus of the tibia. The lateral side of the ankle consists of the much thinner and more delicate fibula.
Figure 1: Surface image of patient’s bruised right ankle.

Activity 1: Classification of Synovial Joints
Materials:
|
Background:
You have 206 bones in your body. Every single one, except for the hyoid bone in the neck region, is connected to another bone. Joints, or articulations, are the meeting points between bones. Joints vary in structure and degree of movement. Joints are classified as synarthrotic (non-mobile and highly stable), amphiarthrotic (slightly moveable) or diarthrotic (freely mobile).
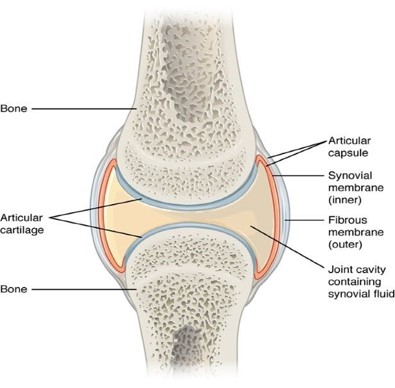
Synovial joints are diarthrotic (or freely moveable). Synovial joints contain a joint capsule filled with synovial fluid (Figure 2). Synovial joints have a few defining characteristics that enable them to have a high range of motion:
- an enclosed cavity lined with an inner synovial membrane producing a viscous fluid called synovial fluid
- articulating bones lined with hyaline cartilage called articulating cartilage at the articulating surface
- a fibrous outer joint capsule
- ligaments and tendons to stabilize the joint
Figure 2: Example of a diarthrotic joint, illustrating parts of the synovial cavity
Diarthrotic joints are also categorized based on their different ranges of motion, and whether the joints do not move around an axis (nonaxial), around a single axis (uniaxial), across two axes (biaxial) or across all three-dimensional planes, (triaxial or multiaxial). To fully understand differences in movements of the joints, carefully analyze the shape of the bones involved, and the location of the muscles, tendons, and ligaments around the joint.
Nonaxial joints do not move around an axis. For example, look at the flat articulating surfaces among the carpal bones. These bones move in a gliding motion past one another, rather than around a particular axis.
Uniaxial (monoaxial) joints move along a single axis. Look at the articulating bones in the elbow between the humerus and the ulna. Notice how the trough shape of the trochlear notch of the ulna cups the cylinder shape of the trochlea of the humerus. This is classified as a hinge joint, like the opening and closing of a door, as it can only move in one plane and one axis (flexion and extension). The knee is another excellent example of a uniaxial hinge joint. Uniaxial joints do not have to be hinge joints. The pivot joint, found in the neck, is another uniaxial joint.
Biaxial joints, like your knuckles, typically have articulations with bones that have rounded edges called condyles; these joints are not as limited in movement as the elbow or the knee. A knuckle is composed of the distal end of a metacarpal bone and the proximal end of the proximal phalange. The distal end of each metacarpal is smooth and rounded, like the bottom of an egg. The proximal surface of each phalange cups the corresponding condyle. The cupping allows your fingers to move in two directions (biaxial movement). 1. You can bend your fingers forward and backward (flexion and extension). 2. The fingers can also move side-to-side as when you spread your fingers out (abduction) and then bring them back together (adduction). The knuckles are categorized as diarthrotic, biaxial joints. They are also referred to as condylar joints. Another biaxial condylar joint is found at the base of the skull, articulating with the atlas (C1) of the vertebrae. A third is found at the ankle, where the talus and distal end of the tibia meet. A unique biaxial joint is the saddle joint, as it does an additional movement called opposition and reposition. The saddle joint is formed by the first carpo-metacarpal joint, thumb.
Helpful Hint:
Abduction: Movement of a body part away from the midline. If you are being abducted you would spread your body out.
Adduction: Movement of a body part toward the midline. If you “add” you bring the structures of your body together.
Multiaxial (or triaxial) joints have the greatest range of movement, determined by their specific anatomical structure and how the bones fit together. For example, the shoulder (acromial joint) and the hip (coxal joint) allow flexion and extension, adduction and abduction, and internal and external rotation. Unfortunately, these highly moveable joints can also be less stable and more prone to injury.
There are other movement types beyond gliding, flexion, extension, abduction, adduction, circumduction, internal and external rotation. They include lateral flexion, dorsiflexion, plantar flexion, eversion, inversion, opposition, reposition, protraction, retraction, and elevation and depression (Figures 3 and 4). There are six types of synovial joints in the body. Each joint has a range of movements permitted based on the shape of the articular surfaces (Table 2).
Table 1: Classification of joint movement and their description.
| Angular or Special | Movement | Description | Opposing Movement |
| A | Flexion | Decreases the angle between bones; brings bones closer together. Movement in an anterior-posterior plane | Extension |
| A | Lateral flexion to the right | The vertebral column moves in the lateral direction along the coronal plane | Lateral flexion to the left |
| A | Abduction | Lateral movement of the body part away from midline | Adduction |
| S | Pronation | Rotation of the forearm where the palm is turned posteriorly (radius rotates over ulna) | Supination |
| A | Dorsiflexion | Ankle joint bends so that the dorsum (superior surface of the foot) moves toward the leg | Plantar flexion |
| A | Inversion | Movement at the ankle joint that turns the sole of the foot medially or inward | Eversion |
| A | Medial or internal rotation | Moving the anterior surface of the limb toward the midline of the body | Lateral or external rotation |
| S | Protraction | Movement of the scapula or mandible in the anterior (forward) direction. | Retraction |
| S | Elevation | Movement of the scapula or mandible in the superior (upward) direction. |
Depression |
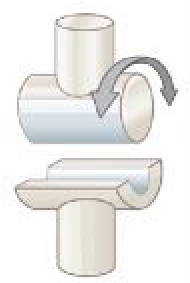
Table 2: The six types of synovial joints, their definitions, and movements.
| Image | Type of Joint | Articular Surface | # of Axes | Movements |
 |
Plane | both surfaces are flat | nonaxial | gliding |
 |
Hinge | convex surface within concave depression | uniaxial | flexion and extension |
 |
Pivot | bone with rounded surface fits into a ligament ring | uniaxial | rotation |
 |
Condylar (Ellipsoidal) Joint | oval, convex surface articulating with concave surface | biaxial | flexion and extension adduction and abduction |
 |
Saddle Joint | convex and concave surface | biaxial | flexion and extension adduction and abduction opposition and reposition |
 |
Ball-and-Socket Joint | spherical head of one bone fitting into cuplike socket | triaxial | flexion and extension adduction and abduction rotation/circumduction |
Figure 3: Movements at diarthrotic (synovial) joints include different forms of flexion and extension (a – d), angular movements such as abduction, adduction, and circumduction (e) and rotational movements (f).
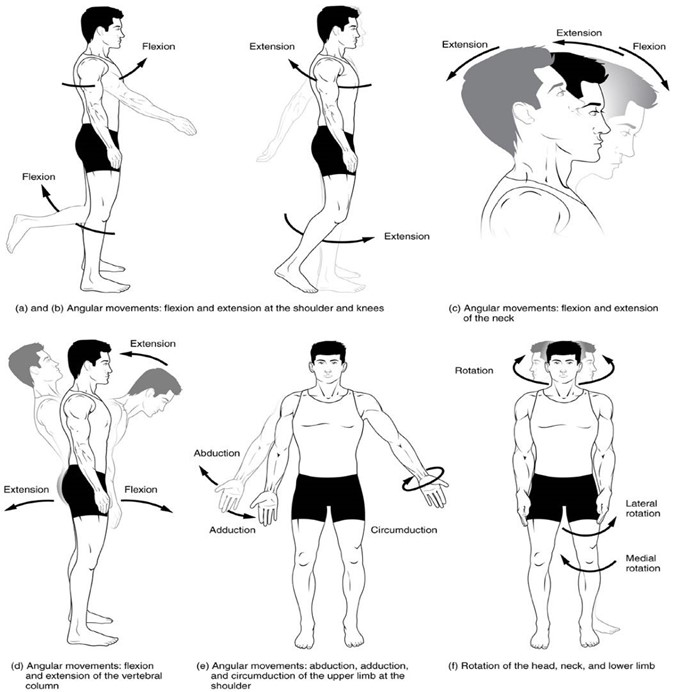
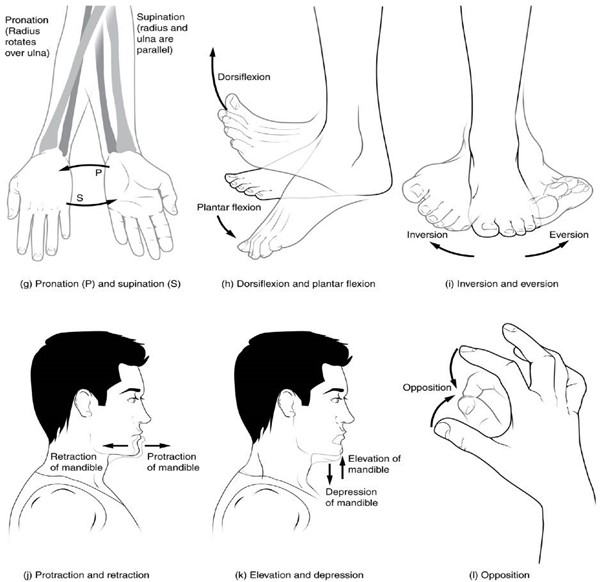
Figure 4: Movements at diarthrotic (synovial) joints include special movements such as supination and pronation (g), dorsiflexion and plantar flexion (h), inversion and eversion (i), protraction and retraction (j), elevation and depression (k), and opposition (l).
A proper evaluation of any patient includes a thorough and systematic physical exam of all major joints to ensure you do not miss any underlying issues. In this case, compensatory injuries are likely to be present in addition to the primary complaint of right ankle pain. Further questioning revels that she has had a prior injury of her left knee that has been bothering her recently.
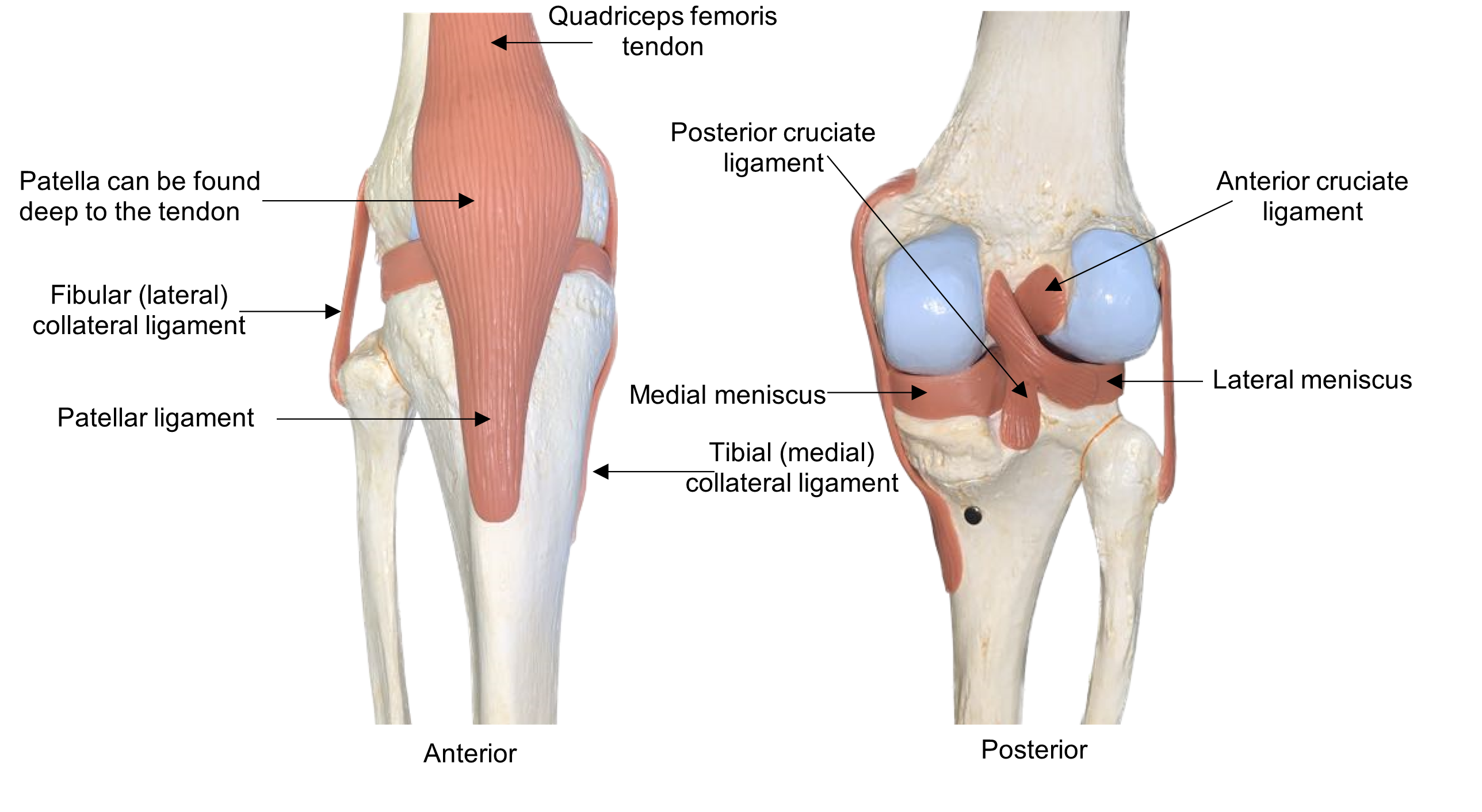
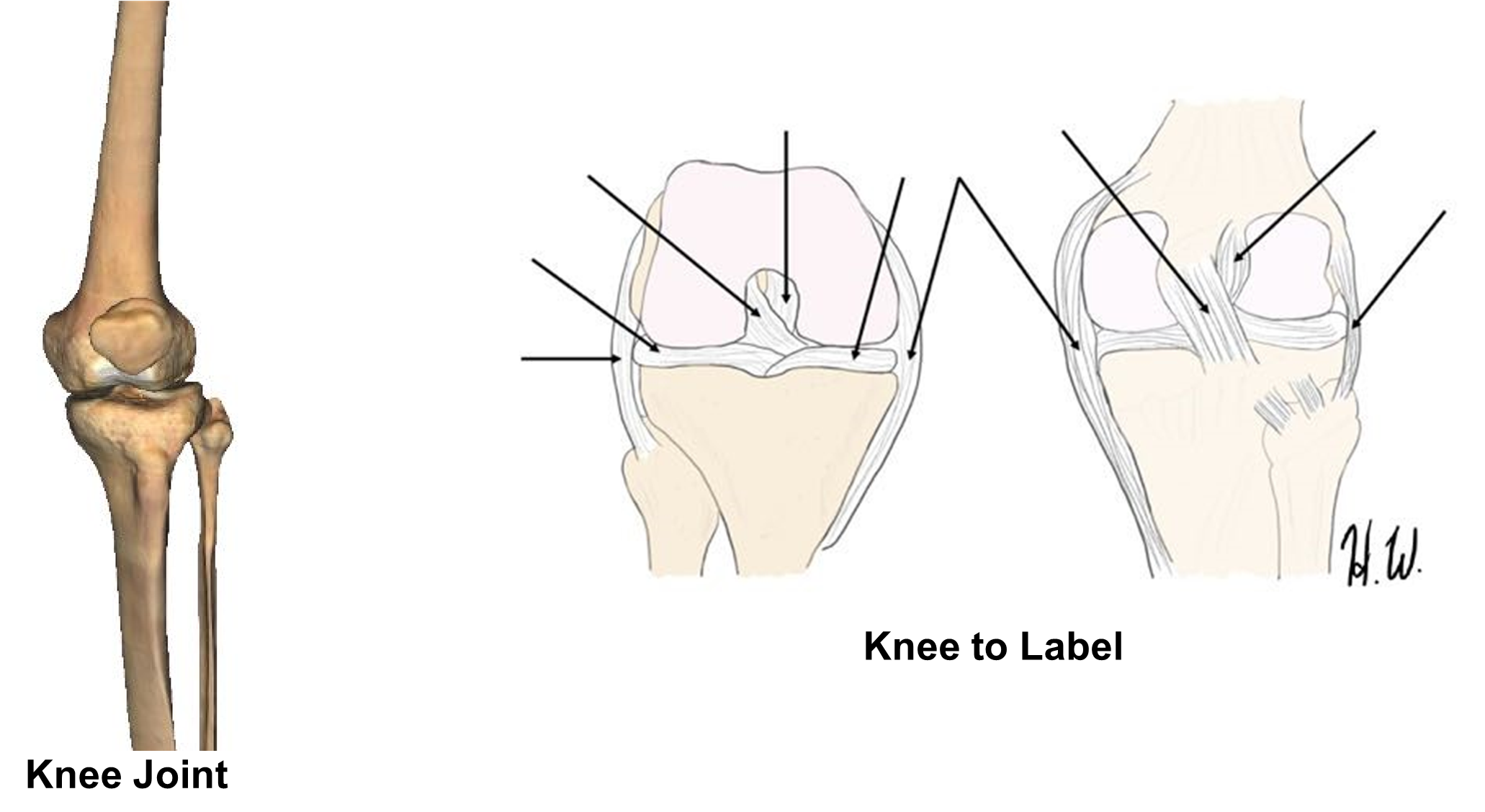
The knee joint is a commonly injured joint. It is the largest diarthrotic joint in the body. It is classified as a hinge joint, but it has a greater range of motion than a simple hinge joint. When the knee is flexed some rotation and lateral gliding movements are permitted. The knee is made up of two joints: the tibiofemoral joint and patellofemoral joint. The patella is a sesamoid and is embedded in the quadriceps femoris tendon. Due to the structure and forces applied to the knee it is one of the more unstable joints. The knee has several extrinsic ligaments to stabilize the knee. The fibular (lateral) collateral ligament and the tibial (medial) collateral ligament provide medial to lateral stabilization of the joint. The two cruciate ligaments, anterior and posterior cruciate ligaments, crisscross and provide anterior to posterior stabilization. Internally, the medial and lateral meniscus made up of tough fibrocartilage deepen the joint to allow for more stabilization of the femoral condyles. They also increase the shock absorbing ability of the joint. (Figure 5)
Figure 5: Anterior and posterior views of the knee model.
For your patient to be able to return to gymnastics without restrictions, all clinical and subclinical injuries must be evaluated and treated. Starting at the most superior joints of the head and neck, you thoroughly assess each joint, asking the gymnast to perform specific movements. This permits you to systematically evaluate her range of motion at all high motion joints. You measure the degree of movement at each joint and note the symmetry between the right and left sides of her body.
Procedure:
- This activity is broken down into stations.
- To understand the movement of a synovial joint, first determine how the bones articulate. Look at the image of the disarticulated and articulated bones provided and examine how they connect. Use the bone articulation shapes to help you classify the joint. Select from the following array of joint types: plane, hinge, pivot, condylar, saddle, or ball-and socket. Remember: the shape of the joint determines the type of movement possible. Then determine the number of axis for each joint. (Table 2)
- On the provided computer or iPad, watch the video of how each joint moves. Bones are unable to move without the aid of muscles. Use the video to help you label the movements of each joint. Then use the letters on the muscle models to help you identify the specific “muscles responsible” for each movement. Hint: Muscles that have similar actions tend to be located together and are innervated by the same nerve. You can use your muscle chart from the muscle lab as an additional resource. Use Table 1 and 2 and Figures 3 and 4 to help fill in the charts.
Station 1A: Atlanto-occipital joint
Look at how the skull and C-1 (atlas) articulate. The occipital condyles of the occipital bone articulate with the superior articular facets of atlas. Note the shape of occipital condyles are like that of a rocking chair. This joint is called a condylar joint. Now move the two bones together. A rocking motion should be observed. This angular motion is described as flexion when the angle between the bones is decreased and extension when the angle is increased. One muscle involved in flexion and extension of the head is the sternocleidomastoid. This muscle originates medially, in the sternal area, and inserts laterally in the cervical area, near the temporal bone. Abduction and adduction are movements seen at condylar joints, but since the neck cannot move toward the midline the movement of the head shifting from side-to-side (laying ear on shoulder on each side) is called lateral flexion.
Bone articulations: Atlas: superior articular facets Occipital bone: occipital condyles
Structural classification of joint: Condylar
# of axis: 1 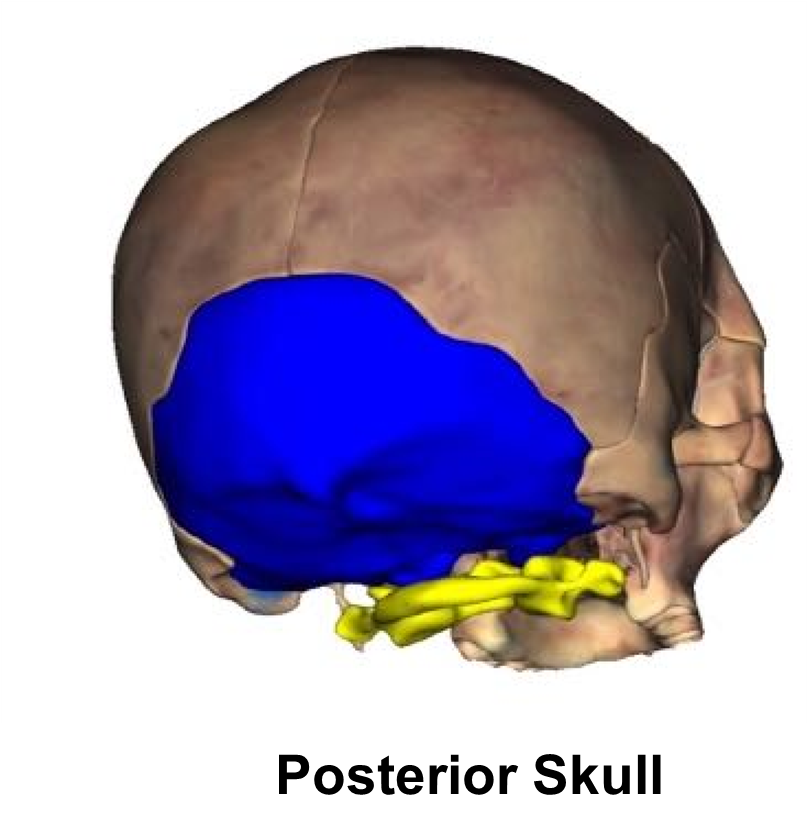
| Motion | Description of Movement | Muscle(s) Responsible |
| A1 | Flexion | a.Sternocleidomastoid |
| A2 | Extension | |
| A3 | Lateral Flexion |
Station 1B: Neck: Atlantoaxial
Bone articulations: Atlas: Anterior arch and Inferior articular facet. Axis: Dens and superior articular facet
Structural classification of joint: _______________________# of axis: ___________
| Motion | Description of Movement | Muscle(s) Responsible |
| B1 | a. |
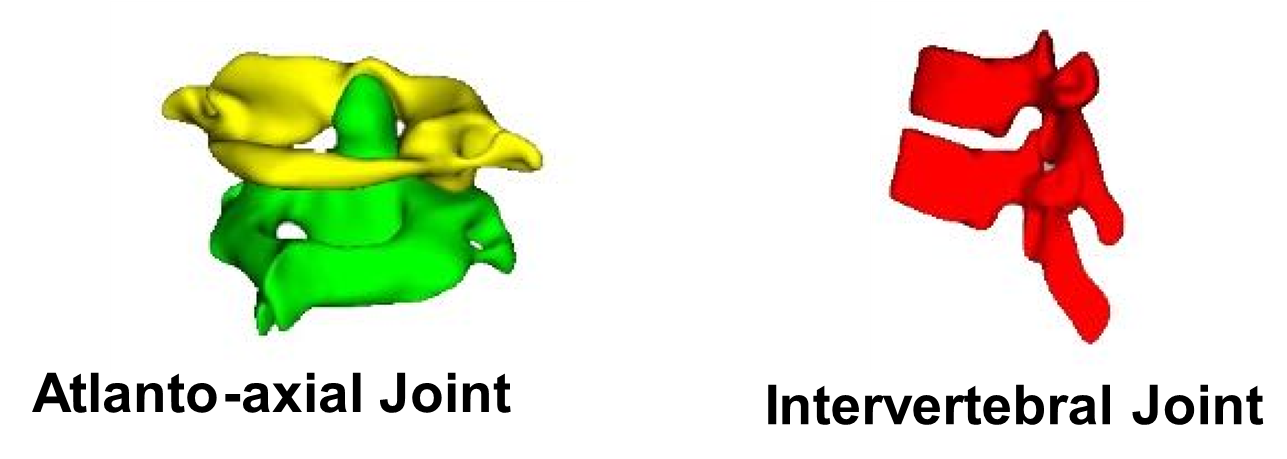
Station 1C: Spine: Intervertebral
Bone articulations: Superior and inferior articular process
Structural classification of joint: ______________________# of axis: ___________
| Motion | Description of Movement | Muscle(s) Responsible |
| C1 | b. | |
| c. | ||
| d. | ||
| C2 | e. | |
| C2 | b. | |
| c. |
Station 2: Glenohumeral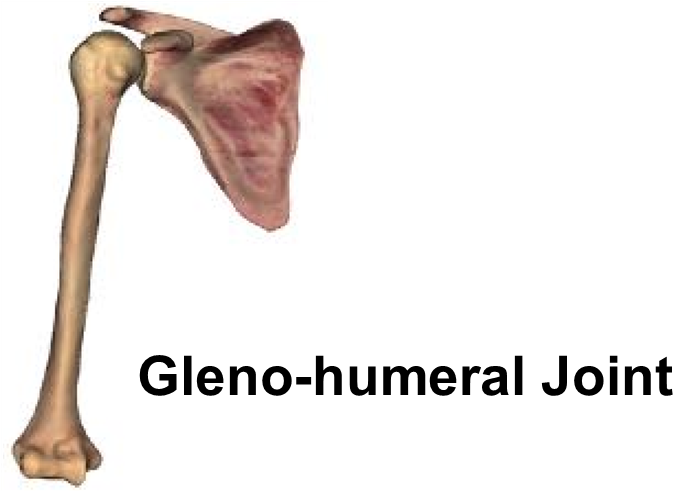
Bone articulations: Scapula: Glenoid cavity, Humerus: head of humerus
Structural classification of joint: __________________
# of axis: ___________
| Motion | Description of Movement | Muscle(s) responsible |
| 1 | a. | |
| b. | ||
| 2 | c. | |
| d. | ||
| 3 | a. | |
| c. | ||
| 4 | a. | |
| d. | ||
| 5 | a. | |
| e. | ||
| 6 | f. | |
| 7 |
Station 3A: Elbow
Bone articulations: *Humerus: Olecranon fossa, coronoid fossa, trochlea, *Ulna: Olecranon process, trochlear notch, and coronoid process
Structural classification of joint: _________________________
# of axis: ___________
| Motion | Description of Movement | Muscle(s) Responsible |
| A1 | a. | |
| b. | ||
| c. | ||
| A2 | d. |
Station 3B: Radioulnar
Bone articulations: *Radius (2 points): Radial head, radial tuberosity, ulnar notch *Ulna: (2 points): Radial notch and head of ulna
Structural classification of joint: _________________________
# of axis: ___________
| Motion | Description of Movement | Muscle(s) Responsible |
| B1 | e. | |
| B2 | f. |
Station 4: Hip (coaxal)
Bone articulations: *Hip: acetabulum * Femur: Head of femur
Structural classification of joint: ________________________
# of axis:___________
| Motion | Description of Movement | Muscle(s) Responsible |
| 1 | a. | |
| 2 | b. | |
| c. | ||
| 3 | d. | |
| 4 | e. | |
| f. | ||
| 5 | d. | |
| g. | ||
| 6 | Tensor fasciae latae | |
| 7 |
Station 5: Knee: Tibiofemoral joint, Patellofemoral joint
Bone articulations: * Femur: Patellar surface, medial and lateral condyle *Patella *Tibia: Medial and lateral condyle
Structural classification of joint: _______________# of axis: ________
| Motion | Description of Movement | Muscle(s) Responsible |
| 1 | a. | |
| b. | ||
| c. | ||
| 2 | d. | |
| e. | ||
| f. | ||
| g. |
Label the image below with the knee joint terms from your terminology list.
Station 6A: Ankle (Talocrural) 
Bone articulations: * Talus, *Tibia: medial malleolus *Fibula: lateral malleolus
Structural classification of joint: ______________# of axis: _________
| Motion | Description of Movement | Muscle(s) Responsible |
| A1 | a. | |
| A2 | b. | |
| c. |
Station 6B: Metacarpo- phalangeal (knuckle)
Bone articulations: metacarpal bone and proximal phalanx
Structural classification of joint: ______________________# of axis: ___________
| Motion | Description of Movement | Muscle(s) Responsible |
| B1 | d. | |
| e. | ||
| f. | ||
| B2 | g. | |
| h. | ||
| B3 | ||
| B4 |
Station 6C: Carpo- metacarpal of digit I
Bone articulations: trapezium and metacarpal I
Structural classification of joint: ________________________
# of axis: ___________
| Motion | Description of Movement | Muscle(s) Responsible |
| C1 | ||
| C2 |
Activity 2: Body in Motion
Materials:
|
Background:
After your thorough physical exam, you observe the following abnormalities: decreased inversion, eversion, and dorsiflexion of the right ankle. All other joints have a normal range of motion. You make a tentative diagnosis: sprain of the lateral ligament of the right ankle. A sprain indicates damage to the ligaments of the ankle joint while a strain would indicate damage to the tendons or muscles. You request an MRI to further evaluate the soft tissues and bony structures of the right ankle.
Recall that anatomical position is defined as the body and head being forward facing, standing upright, with palms facing forward, feet shoulder width apart, and toes pointing forward. Now you will apply what you have learned about articulating bones, joint movement, and muscle action on a figure (image) of a body in motion.
Procedure:
- Look at the given description. In the space below, please move the jointed body into the positions listed in the table below. Then draw a stick figure of your model.
| Joint | Position | |
| Neck: Atlanto-occipital | Extension | |
| Neck: Atlantoaxial | AP | |
| Spine: Intervertebral | Lateral flexion | |
| Joint | Right Side of Body | Left Side of Body |
| Glenohumeral | Abduction | Abduction |
| Elbow | Extension | Extension |
| Radioulnar | Supination | Supination |
| Hip (coaxal) | Abduction | Abduction |
| Knee: Tibiofemoral joint/Patellofemoral | Extension | Extension |
| Ankle (Talocrural) | AP | AP |
| Metacarpo-phalangeal (knuckle) | Adduction | Adduction |
| Carpo-metacarpal of digit I | Adduction | Adduction |
2. Using the image provided, fill in the chart below. If the joint is in Anatomical Position write “AP” in the space provided and describe the position (extension of knee, for example).
| Joint | Position | 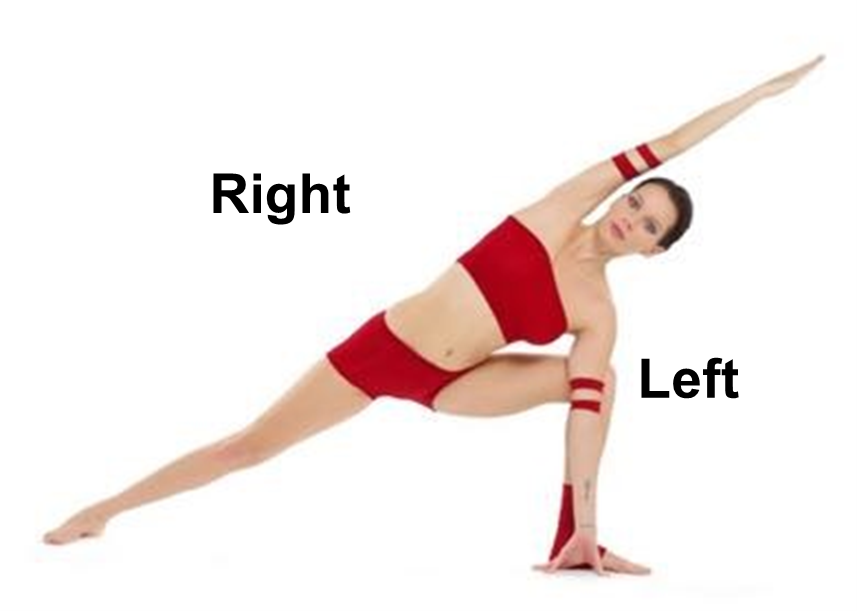 |
| Neck: Atlanto-occipital | ||
| Neck: Atlantoaxial | ||
| Spine: Intervertebral | ||
| Joint | Right Side of Body | Left Side of Body |
| Glenohumeral | ||
| Elbow | ||
| Radioulnar | ||
| Hip (coaxal) | ||
| Knee: Tibiofemoral joint/Patellofemoral | ||
| Ankle (Talocrural) | ||
| Metacarpo-phalangeal (knuckle) | ||
| Carpo-metacarpal of digit I |
Putting it All Together
The MRI results confirm a right ankle sprain. The patient’s ankle will experience tremendous swelling (inflammation) and pain for the next week or two. She must rest the ankle and reduce the inflammation as much as possible. She will do this by compressing the ankle in a supportive wrap and keeping it immobile, and by icing the area several times a day. She can also take a non-steroidal anti-inflammatory drug (NSAID) to reduce pain and swelling. Elevating her foot above her head will help the excess fluid to drain away from the injury, reducing swelling. Together, the rest, ice, compression, and elevation form the acronym RICE. After 6-8 weeks (about 2 months) of physical therapy, her ankle should be much better, and she should be able to bear weight again.
Creative Commons Citations:
- Joints lab. Case Based I OER Lab Manual for A&P I. © 2022 by G. Backus, H. Wangerin, and P. Rodgers is licensed under CC BY-NC-SA 4.0.
- Figure 1 and 5 © 2023 by H. Wangerin are licensed under CC BY-NC-SA 4.0
- Figures 2, 3, 4, and images in table 2 © 2022 OpenStax Anatomy and Physiology 2e licensed under CC BY 4.0
- Posterior Skull, Atlanto-axial Joint, Intervertebral Joint, Gleno-humeral Joint, Elbow Joint, Radioulnar Joint, Hip Joint, Knee Joint, Ankle Joint, Hand Joints, Thumb Joint © 2023 by H. Wangerin, using the Anatomage Table, are licensed under CC BY-NC-SA 4.0
- Body in Motion 1 and Body in Motion 2 © Nina Mel is licensed under CC BY 3.0 Wikimedia commons some rights reserved license by Nina Mel: Body in motion, and Body in motion 2 (https://commons.wikimedia.org/wiki/File:Utthita-Parshvakonasana_Yoga-Asana_Nina-Mel.jpg)
